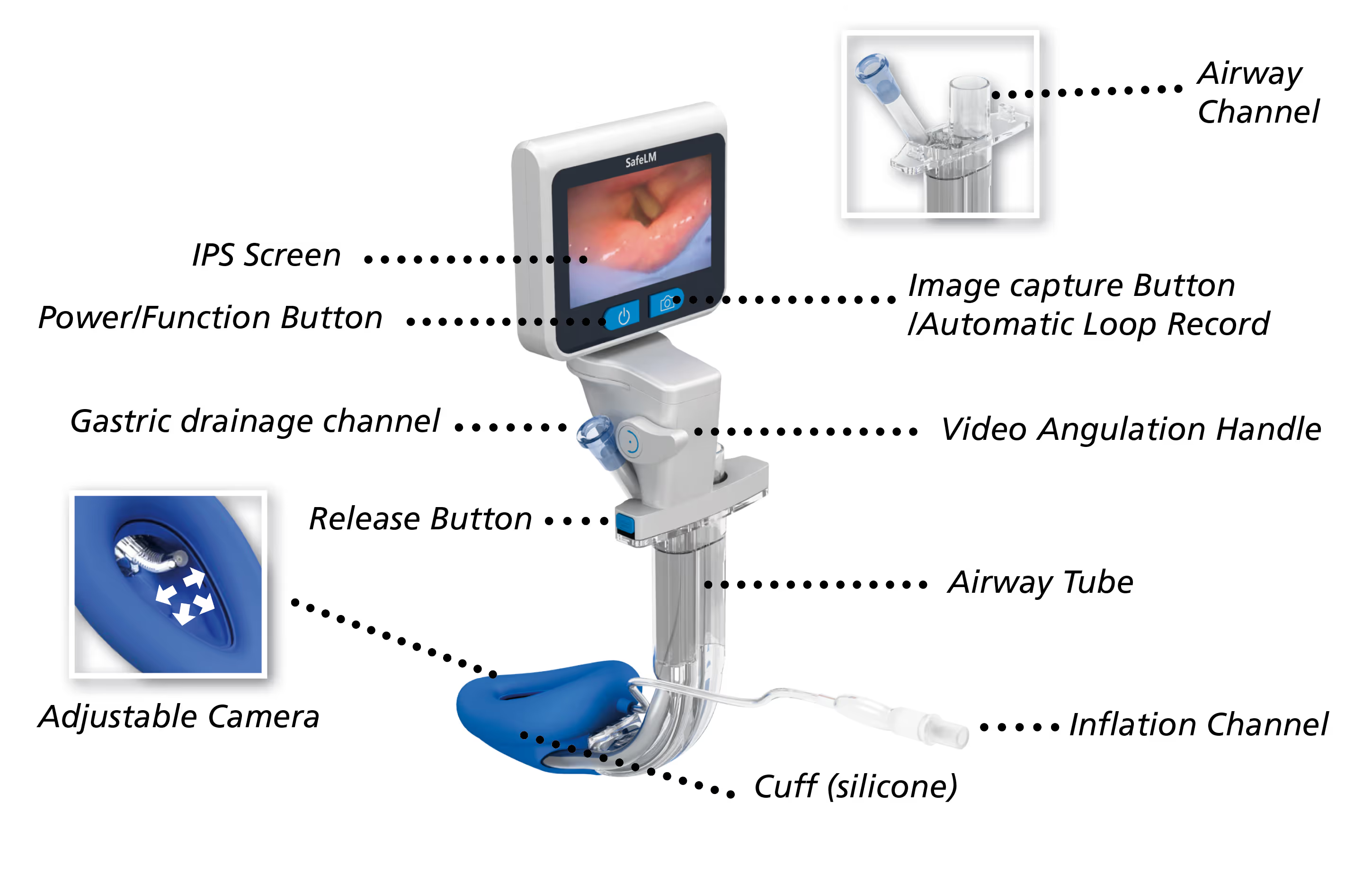
SafeLM



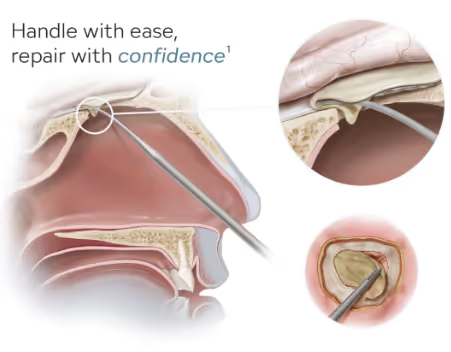
Supraglottic airways (SGAs) are well established in modern anaesthetic practice. Yet, despite their recognised advantages over endotracheal intubation in appropriately selected patients, they are still often reserved for shorter and less demanding procedures.
One reason, reported in the BJA1, is that blind placement may be suboptimal, which can reduce clinician confidence when considering SGAs for longer cases or more complex patient positioning.
SafeLM® videoscope

SafeLM® has been designed to address this challenge by combining supraglottic airway management with continuous visualisation. For selected patients, this may support a more controlled airway strategy while retaining the recognised benefits associated with avoiding routine endotracheal intubation in every case.
At a glance
- Visual placement with continuous airway monitoring
- Real-time visualisation and management of secretions above the cuff and within the gastric channel, whilst oxygenating
- An Oropharyngeal Leak Pressure (OLP) of 35-40 H2O is possible with the SafeLM, supporting use in longer cases, selected laparoscopic procedures and non-supine positions, including Trendelenburg
- A conduit to intubation, if escalation is required
- Potential to reduce intubations as routine, in selected cases
- Supports enhanced patient recovery principles, that can contribute to theatre efficiencies
Pushing the boundaries of SGA use
Evidence-informed. Clinically grounded.
SafeLM® builds on the evidence base supporting modern second-generation supraglottic airways, while adding continuous visualisation and a conduit-to-intubation capability.
Key published evidence includes:
- Van Zundert et al1,2. reported that blind SGA placement is suboptimal in 50-80% of cases, highlighting the potential value of direct visualisation.
- Park et al6. found that, in selected laparoscopic cases, SGAs were associated with fewer postoperative airway complaints and comparable ventilatory performance when compared with endotracheal tubes.
- Schwartz and Peng3. described second-generation SGAs as a safe option for appropriately selected laparoscopic procedures, with potential advantages in haemodynamic response, airway morbidity and recovery.
- Geng et al8. (2025) reported smaller haemodynamic changes with SafeLM® than with endotracheal intubation during arthroscopic shoulder surgery.
SafeLM® - designed to help anaesthetists confirm placement, maintain visual control of the airway throughout the case, and expand the use of SGAs in appropriately selected patients with greater confidence.
Further Information
References
1. A. A. J. Van Zundert et al, Malpositioning of supraglottic airway devices: preventive and corrective strategies British Journal of Anaesthesia 116 (5): 579–82 (2016)
2. A. A. J. Van Zundert et al, The case for a 3rd generation supraglottic airway device facilitating direct vision placement. Journal of Clinical Monitoring and Computing (2021) 35:217–224
3. Schwartz S, Peng YG. Supraglottic airway devices (SADs) and laparoscopic surgery. APSF Newsletter. 2023;38:18–19.
4. Clístenes Crístian de Carvalhoet al. Second-Generation Supraglottic Airway Devices Versus Endotracheal Intubation in Adults Undergoing Abdominopelvic Surgery: A Systematic Review and Meta-Analysis. IARS February 2025 • Volume 140 • Number 2
5 André A. J. Van Zundert et al. The case for a 3rd generation supraglottic airway device facilitating direct vision placement. Journal of Clinical Monitoring and Computing (2021) 35:217–224
6. Park SK, Ko G, Choi GJ, et al. Comparison between supraglottic airway devices and endotracheal tubes in patients undergoing laparoscopic surgery: a systematic review and meta-analysis. Medicine (Baltimore).2016;95:e4598.PMID:27537593.
7. Carron M, Veronese S, Gomiero W, et al. Hemodynamic and hormonal stress responses to endotracheal tube and 6 ProSeal Laryngeal Mask Airway™ for laparoscopic gastric banding. Anaesthesiology. 2012;117:309–320.
8. Geng CJ, et al. Use of view-adjustable video laryngeal mask versus endotracheal intubation for airway management during anaesthesia for arthroscopic surgery: a randomized trial. Annals of Medicine. 2025;57(1):2519683.
Tel: 01264 332172
Email: info@CCMed.co.uk
We hope you found the videos of interest. To learn more or request a demonstration please contact us on 01264 332172, email info@ccmed.co.uk or use our contact form.